
Health Infrastructure
Overview of healthcare infrastructures (PATH)
The Nicaraguan healthcare system is divided into tiers of care, kind of like a web, and functions through a bottom-up approach. MINSA, the “Ministerio de salud,” is the primary health provider in Nicaragua, covering around 70% of the population. The Nicaraguan Social Security Institute (INSS) covers formal sector workers and finances health care for about 10% of the population. The rest of the population receives healthcare from private services.
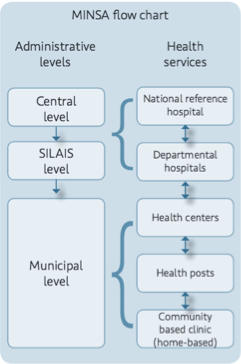
Figure 1. MINSA flow chart
MINSA (PATH)
MINSA functions both as a regulatory agency and as a provider of health services.The regulatory role is filled by MINSA central, while the provider role is filled by the 17 departmental SILAIS (Sistema Local de Atención Integral En Salud), which make up a network of 1,059 health facilities. At the SILAIS level, work is coordinated by a director and senior management team that includes the heads of financial/administrative services, health services, health surveillance, regulatory affairs, human resources, and labor union representatives. Work in each municipality is coordinated by a municipal director and a senior management team, which is comprised of a nursing chief, manager, epidemiologist, and doctor responsible for health care services.
Network of health facilities (PATH)
The national service network is made up of 1,059 health care units, consisting of 32 public hospitals, 28 health centers with beds, 144 health centers without beds, and 855 health posts.
Hospitals (PATH)
21 of the hospitals are departmental reference hospitals, providing impatient care in internal medicine, pediatrics, obstetrics/gynecology, surgery, and orthopedics. Other services include emergency care, specialty outpatient care, clinical laboratory services, pharmacy services, and imaging. Most hospitals are on the pacific side, and there are only three hospitals in the Caribbean region. The average hospital coverage is one hospital per 212,800 people, but there is a wide variation depending on location. Resource availability at each hospital varies, and hospitals in many areas are often hard to get to for people living in more remote regions.
Health Centers (PATH)
Health centers are staffed by practitioners or nurses, and offer primary health care services. Primary health care services include: pharmacy, basic laboratory, immunization, mental health services, zoonosis care, environmental health services, and sometimes dentistry. Most have emergency departments, and some have gynecology and pediatric outpatient consultations. Most are located in the pacific and central regions of the country, with minimal access for the Caribbean region. The average coverage of a health center with inpatient capabilities covers 170,000 people, and the average coverage of a health center without beds covers about 36,000 people. Once again, these numbers vary greatly depending on the location of the center.
Health Posts (PATH)
There are 855 health posts in the nation of Nicaragua, and they are under the jurisdiction of individual communities. They are staffed by one or two nurses, and sometimes a doctor. Health posts deliver primary health care and work on health promotion and disease prevention. The specific activities this translates into are: comprehensive health care for women and children, health care for general morbidity, community education, primary emergency care, immunizations, epidemiological surveillance, pharmacy services, and the completion of various statistical information forms. Some also provide rapid malaria or HIV/AIDS testing. Each health post serves about 6,400 people, however the dispersion of the rural population in large territories such as the RAAN and RAAS leads to less efficient coverage by health centers and health posts.
Community-Based Health Network (PATH)
The nation-wide community based health network includes about 4,400 home-based community clinics and 33 Casa Maternas. There is an impressive network of MINSA-trained independent volunteers, including 12,700 “brigadistas,” 6,200 midwives, 7,100 “voluntary collaborators,” 2,800 health promoters who link NGO efforts, and 340 health representatives on community boards that are linked to the municipal governments. All of these workers promote health at the community level with no compensation from MINSA.
Casa Maternas
Casa Maternas (Maternal Homes) are short-term residence establishments that are available for women in more rural and remote areas to come to in the weeks preceding birth. They are excellent resources for mothers in rural areas who do not have access to other forms of care. The Casa Materna provides these women with food, shelter, education, transportation, and obstetrics care.[3] Most births will take place at a nearby hospital, but births can also happen in the Casa Materna.
Bridges to Community Casa Materna
Construction of the Casa Materna in Hormiguero near Siuna began on February 17th, 2014.
“I think what stood out to me the most was the participation of the community members in the construction. People traveled for an entire day by foot to help. We realized then the real importance of the maternity house–how much these communities needed it.” -Apolinar Centeno, Project Coordinator, Siuna The idea for the Siuna Maternity […][4]


Images: Bridges To Community Casa Materna in Hormiguero
MINSA-trained independent volunteer types: (PATH)
Brigadistas
- Providing community-based education and health outreach
- Through home visits, identifying and referring pregnant women, girls needing family planning, malnourished children, and children in need of immunization
- Identifying and referring patients to health units, with emphasis on children and women
- Reporting deaths and referring and reporting potentially communicable diseases
- Conducting a community census
- Providing support for national health campaigns (immunization, anti-epidemic days), within their communities. Encouraging people to participate, arranging locations for developing these activities locally, and helping manage medical inputs such as antiparasite medicine, antilice medicine, and oral rehydration solution
- Weighing children monthly as part of a community-based activity called PROCOSAN
- Administering contraceptives to local women previously registered for this program in the health units
- Monitoring patient progress in accordance with referrals made by health units
Voluntary collaborators (“col-vols”)
- Managing suspected cases of malaria, including conducting a rapid diagnostic strip test, whenever available, or creating a thick smear slide for diagnosis at local health unit
- Administering antimalarial sanitation measures such as elimination of mosquito-breeding sites
- Educating the public about malaria prevention
- In some cases, using or distributing basic medical input stock such as oral rehydration solution, acetaminophen, and chlorine for water disinfection
Midwives
- Identifying and referring pregnant women for prenantal services and health-facility based delivery
- Keeping a local census of pregnant women
- Monitoring the delivery plan for pregnant women in their community
- Providing health care services for uncomplicated deliveries
- Promoting family planning methods
Health care professionals:
- The Nicaraguan Ministry of Health provides no financial incentives for health care staff to work in remote and difficult-to-access areas.
- There is less than 1 physician per 1,000 inhabitants, with the lowest levels of health care coverage found in rural areas.
- Nicaragua does not train personnel to carry out any health promotion activities
(Doctors for Doctors http://www.doctorsfordoctors.ca/dfdrural-nicaragua)
Human resources: 4.5 doctors, 3.4 registered nurses, 7.1 auxiliary nurses, 9.2 available beds per 10,000 people. Average annual number of ambulatory care visits is 1.9 per inhabitant with 1.3 medical consultations per inhabitant
- Distribution of health workers varies
- 65% Pacific Coast Region
- 16% Central Zone
- 10% Northern zone
- 9% Caribbean region
- Salaries for MINSA health staff are significantly lower than those in neighboring countries, providing little financial incentive and even less incentive to go work in remote areas
- Lack of infrastructure needs:
- 35% of health facilities do not have access to electricity
- 45% do not have water
[3] http://www.borgenmagazine.com/improving-maternal-child-health-in-nicaragua/
Am an Emergency Medical Technician, EMT from Ghana and I will like to come and assist in your health services. If only am invited.
Thank you.